At the 2016 OARSI World Congress in Amsterdam, Netherlands, Dr. Neil Segal, MD, MS, and Dr. Ali Guermazi, MD, PhD , presented a poster describing “Advances In Visualization Of Knee Cartilage And Meniscus With Standing Computed Tomography Arthrography”.
Standing CT arthrography (SCTa) has also been shown to have some distinct advantages over MRI, according to the poster presentation. “Potential advantages of SCTa over non-weight-bearing MRI/MRA include: 3D measures of meniscal position and morphology; detection of pathology not detected in unloaded positions; and ability to bear weight bilaterally in a functional position, better recreating the magnitude of muscle and external forces acting about the knee during usual standing…. SCTa can be obtained in multiple knee flexion angles, while an MRI knee coil may permit imaging only with the knee in extension, and SCTa is less expensive than MRI.”

As part of the background for their presentation, Drs. Segal and Guermazi stated that “MRI is the standard for non-invasive visualization of cartilage and menisci, and … Absence of weight bearing limits evaluation of the functional position and configuration of these structures…Advances in standing CT (SCT) have allowed 3D imaging of the knees while under physiological loads, similar to fixed-flexed or semi-flexed radiograph protocols.”
Their objective was to evaluate a protocol for SCTa for imaging weight bearing cartilage and menisci and to assess potential advantages over non-weight bearing MRI.

Although the sample size was small, the results were noteworthy. As shown in the images, SCTa permits evaluation of cartilage and menisci in three dimensions, while the patient is standing and under physiological load. Furthermore, SCTa, “may be useful for assessment of menisci as well as tibiofemoral and patellofemoral cartilage in functional stance,” according to the presentation.
The two participants in the study were a 42-year-old man without osteoarthritis (Figures 1 and 2), and a 67-year-old woman with KL2 knee osteoarthritis (figures 3-5). The participants had a similar contrast agent applied.
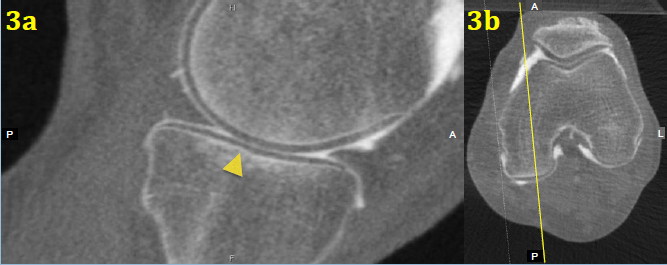
Figure 3b: Axial image depicting location of the sagittal slice in Figure 3a
The actual imaging techniques used were fixed-flexed (approximately 20°) SCTa (INVESTIGATIONAL ONLY cone beam CT knee imaging system*, CurveBeam, Warrington, PA, USA) and non-weight bearing MRI (Siemens TrioTim, Washington DC, USA).
“Following 2-3 minutes of unloaded knee flexion and extension, a low-dose SCT scan was acquired utilizing cone beam reconstruction. Participants were positioned with the tips of the great toes, patellae, and the anterior superior iliac spines coplanar to each other and the feet 10°externally rotated. Scans were acquired with a 0.3mm isotropic voxel size (20x 35x35cm) with an effective radiation dose of approximately 0.1 mSv. 10 minutes following SCTa, MR arthrography was acquired (NEX=1, ETL=3, Slice thickness=2 mm, Slice spacing 2 mm, Matrix= 240 x 320, FOV=140 mm with axial T1 fat-sat (TR=712 msec, TE=12 msec); coronal T1 fat sat (TR=730 msec, TE=10 msec); and sagittal T1 fat sat (TR=796 msec, TE=10 msec).
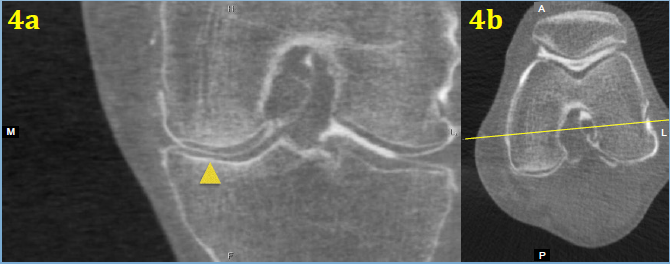
Figure 4b: Axial image depicting location of coronal slice in Figure 4a
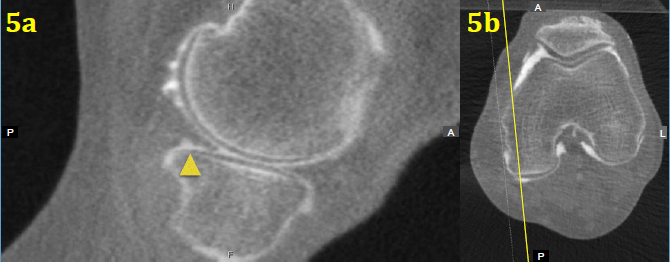
Figure 5b: Axial image depicting location of sagittal slice in Figure 5a
*The CurveBeam knee imaging system is investigational only and is not available for sale in the US.