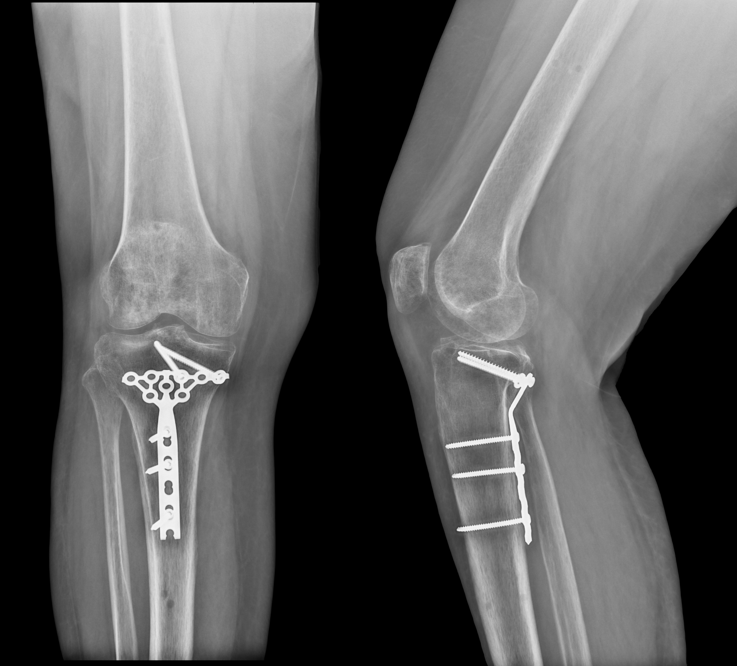
X-rays of knee may not always provide accurate post-operative assessments. For example, in the case below, post-operative X-Rays suggested a posterior shear tibial plateau fracture had been sufficiently healed.
Post-operative X-Rays appeared to show a healed posterior shear tibial plateau fracture.
However, a CurveBeam LineUP weight bearing CT exam of the same patient showed a portion of the fracture had not fused as desired.
The weight bearing CT scan revealed a portion of the fracture had not yet healed.
The LineUP provides three-dimensional views of fractures. The treating physician for this case, Dr. Blake Moore, said weight bearing CT has been the most critical addition to his practice since he began it, adding that it “greatly enhances the level of care and sophistication of preoperative planning.”
Are you attending the SSR Annual Meeting? Be sure to visit CurveBeam’s exhibit to learn more about weight bearing CT imaging and how it is revolutionizing orthopedic medicine.
Midfoot arthritis is a challenging problem that causes foot pain and can impede daily activity. Surgery, specifically midfoot arthrodesis, is considered when initial conservative management fails. Arthrodesis should be limited to the symptomatic joints, but it is often difficult to determine which joints are causing the symptoms. Precise anatomic preoperative diagnosis is essential (1).
Cone Beam CT imaging can assist surgeons in understanding complex forefoot deformities and devising the appropriate surgical plan.
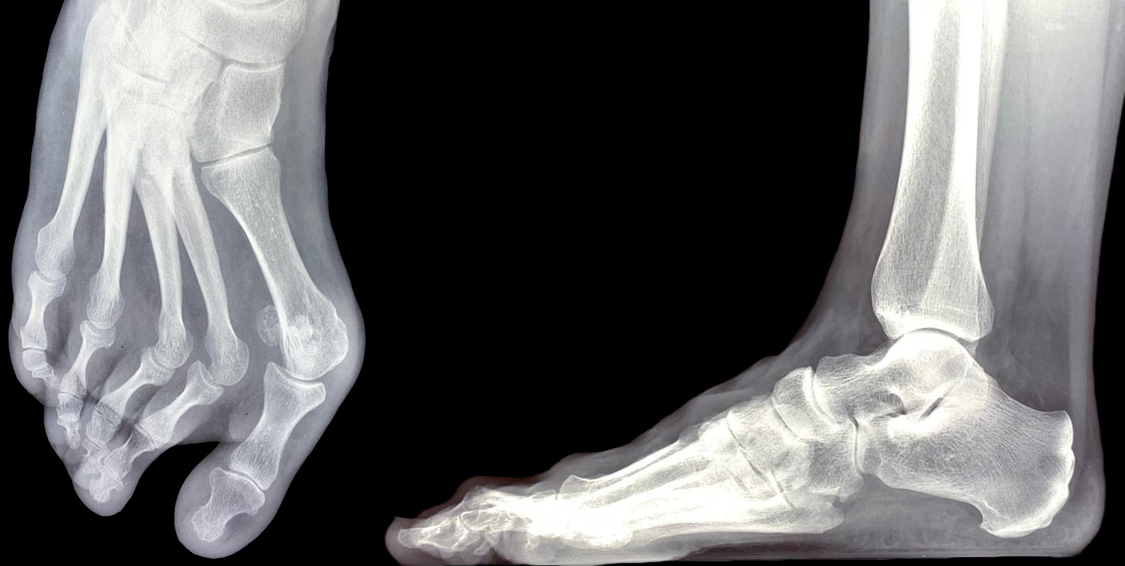
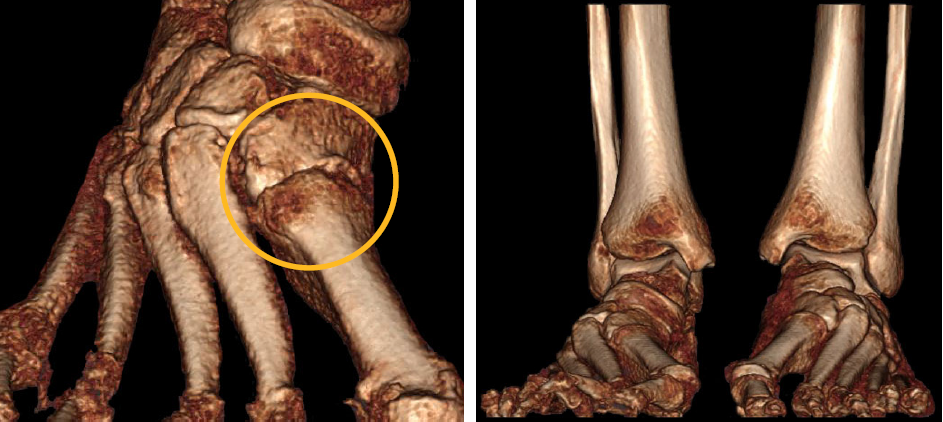
For example, in the case below, a patient presented with forefoot pain and was a candidate for surgical revision after X-Ray exams revealed a forefoot deformity.
The patient’s X-Ray displayed a complex midfoot deformity, however the anatomy was too superimposed on the lateral X-Ray to understand the functional position of the tarsometatarsal joints.
Based off of the X-Ray images alone, the treating doctor would have performed a scarf osteotomy and Weil procedures on the 2nd and 3rd metatarsals.
A follow-up weight bearing cone beam CT scan via a CurveBeam pedCAT was ordered.
Sagittal MPR slices revealed 1st tarsometarsal gapping and 2nd tarsometatarsal degeneration.Joint degeneration, as well as instability of the 1st, 2nd and 3rd tarsometatarsal joints, was more apparent on the 3D renderings.
Based on the weight bearing CT scan, the surgical plan was revised to a Lapidus bunionectomy and a 2nd and 3rd tarsometarsal joint arthrodesis.
Will you be attending the AAOS Annual Meeting in Orlando? Visit CurveBeam at Booth #2909 to learn more about weight bearing cone beam CT imaging.
(1) Verhoeven N, Vandeputte G. Midfoot arthritis: diagnosis and treatment. Foot Ankle Surg. 2012;18(4):255–262. doi:10.1016/j.fas.2012.04.004
A loose body is a bone or cartilage fragment that has chipped off inside a joint. If left in place, a loose body can damage a joint surface, cause pain, and restrict movement.
A 2D radiograph is typically the first test performed when looking for a loose body, but overlapping bone may obscure loose bodies. Cone Beam CT imaging provides a 3D image of the foot & ankle at a dose comparable to 2D imaging.
Dr. Albert Armstrong, DPM, MS, BSRS, Professor of Radiology and Medical Director of Advanced Imaging at the Barry University School of Podiatric Medicine, shared such a case in a recent FOOTInnovate lecture.
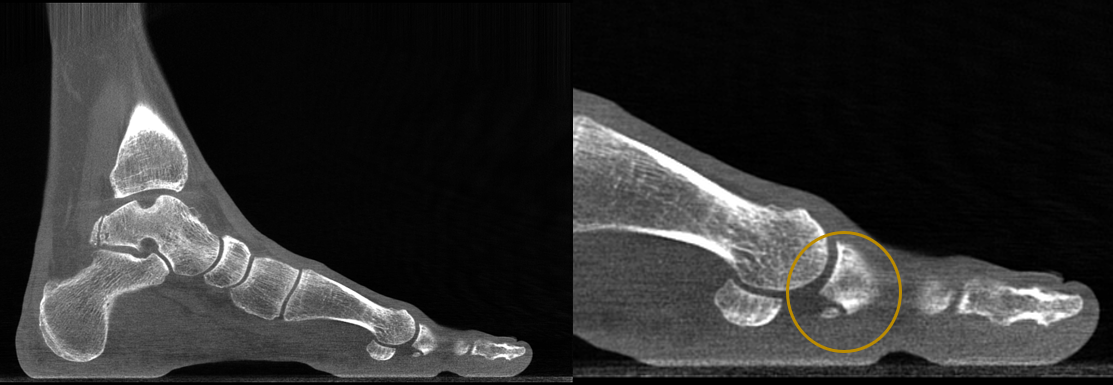
A 38-year-old male patient presented with pain in his left foot, mainly in the great toe. He said his toe felt stiff and would often “lock up.”
A 38-year-old patient presented with pain in his great toe. Due to bony overlap, 2D radiographs were inconclusive as to the cause of pain.
A cone beam CT scan was ordered as a follow-up exam. Because the podiatric clinic at Barry University has a CurveBeam pedCAT on site, the patient was able to get the scan immediately.
The sagittal MPR slices revealed osteophyte formations on the 1st MTP joint, and a resulting loose body.
The cone beam CT scan revealed osteophyte formations on the 1st metatarsophalangeal joint, and a resulting loose body.
Osteochondral lesion of the talus is a broad term that describes injury or abnormality to the talar articular cartilage and adjacent bone. Researchers have shown that radiographs alone miss osteochondral lesions of the talus in up to 50 percent of patients (1) .
Dr. Albert Armstrong, DPM, MS, BSRS, Professor of Radiology and Medical Director of Advanced Imaging at the Barry University School of Podiatric Medicine, shared such a case in a recent FOOTInnovate lecture.
A 40-year-old male patient presented with pain in his left ankle. He was a self-described tough guy who said he has been tolerating the pain for years, but his new job required him to be on his feet all day.
The patient’s X-Rays showed a previous avulsion fracture and some radiolucency in the talar dome, but were otherwise inconclusive:
This 40-year-old male patient’s X-Ray revealed a previous avulsion fracture and some radiolucency around the talus, but was otherwise inconclusive as to why the patient was suffering ankle pain.
A weight bearing CT study was ordered, and it clearly showed two osteochondral lesions in the talar dome, as well as an osteophyte formation on the anterior ankle. Both of these findings pointed to osteoarthritis in the ankle.
The CurveBeam weight bearing CT scan revealed two osteochondral lesions as well as an osteophyte formation on the anterior ankle.
Large lesions and bipolar lesions associated with advanced degenerative joint disease do not respond to simple debridement or cartilage resurfacing techniques. In a case featured in Podiatry Today, a weight bearing CT scan taken after standard X-Rays of a 52-year-old patient with chronic right ankle pain revealed large subchondral cystic changes and bipolar lesions. After reviewing the X-Ray and weight bearing CT. doctors determined the patient to be a good candidate for a total ankle replacement.
Will you be in San Antonio for the ACFAS Scientific Conference Feb. 19 – 22? Visit CurveBeam at exhibit #407 to see several more examples of how weight bearing CT can provide more detailed diagnostic information than X-Ray alone.
(1) Badekas T, Takvorian M, Souras N. Treatment principles for osteochondral lesions in the foot and ankle. Int Orthoped. 2013; 37(9):1697-1706.
The WBCT Society presented another Open Scientific Meeting on September 13, 2019 at the AOFAS Conference in Chicago. Watch the highlight reel from the meeting above to see some of the key moments or read the summary below!
The WBCT Society is an independent research organization. CurveBeam is a proud sponsor of the Society.
New Leadership:The WBCT Society presented Dr. Martinus Richter, MD, PhD, a plaque for serving as founding president. Dr. Richter’s term ended at the meeting, and incoming president Dr. Alexej Barg, MD, assumed the role.
Semi-Automatic 3D Hindfoot Measurements: Dr. Alessio Bernasconi discussed a study that demonstrated semi-automatic 3D hindfoot alignment measurements were reliable when measuring alignment on pes cavo-varus cases.
New Research Protocols: Dr. Alexandre Godoy, MD, demonstrated how the University of Sao Paulo in Brazil has designed three new research protocols for its CurveBeam LineUP weight bearing CT system. These include:
Cavus varus deformity: perform a Coleman block test clinically and during weight bearing CT to determine if the Coleman block test changes alignment measurements.
Hallux valgus deformity: use weight bearing CT to assess 1st TMT gapping, collapse of medium column, and 1st MT and sesamoid rotation.
Congenital club foot: Investigate residual club foot using WBCT to try to understand relationships between tarsal bones involved in the deformity.
The optimal workflow for in-office Weight Bearing CT (WBCT) imaging is to get insurance authorization, perform the scan, and review scan results all during the initial patient appointment.
Hallux valgus is a tri-plane deformity, and weight bearing allows for a better understanding of coronal plane rotation.
Post-operatively, weight bearing CT can provide a precise view of the rate of fusion healing.
The webcast covered the importance of weight bearing in foot and ankle imaging, the applications of weight bearing CT in common foot and ankle disorders, and how it can be incorporated effortlessly into practices.
According to Dr. Cuttica, “Weight bearing is the functional position of the foot. It allows for us to better determine alignment, to form an assessment of the foot, and to formulate treatment plans. So, weightbearing, obviously as we all know, is very, very important.”
A surgeon at Orthopaedic Foot & Ankle Center (OFAC) in Falls Church, Virginia, Dr. Daniel J. Cuttica, DO, boasts a number of specialties and interests, including foot and ankle surgery, reconstructive surgery, sports-related foot and ankle disorders, cartilage disorders, total ankle replacement, diabetic limb salvage, and dance medicine.
Background
Dr. Cuttica states, “When you evaluate a patient, in addition to clinical exam, you know that imaging is going to be very valuable in diagnosing, treating, and assessing outcomes in foot and ankle.”
However, with weight bearing imaging, you can more reliably identify pathology such as subtle arch collapse, loss of cartilage/joint space, degenerative changes, and impingement.
The Limitations of Conventional CT vs. the Benefits of WBCT
When compared to plain X-Rays, “Computed Tomography (CT) can be very, very beneficial for bone and joint problems, and it does give us a large amount of additional information.” However, Dr. Cuttica explains, “The biggest limitation, at least in foot and ankle, with CT again, is probably your inability to obtain weight bearing images.”
The benefits of CBCTs include:
Easy to operate
Shorter scan time
Patient safety
Optimal patient positioning
Offloads capacity
Flexible siting/easy relocation
There are also many advantages to using WBCT, including:
Ability to obtain weight bearing images
High contrast and spatial resolution
Fast image acquisition time
Decreased radiation (typically 0.01-0.03 mSv vs. 0.07 mSv for Conventional CT)
Relatively small scanner size with portability
Less capitalization cost than Conventional CT
Implementing In-Office WBCT for Foot & Ankle
According to Dr. Cuttica, because of its low radiation dosage and small size, CBCT is ideal for an office setting. For patients, a WBCT scanner in the office is more convenient, can help to avoid unnecessary follow up appointments, and allows for immediate feedback of their diagnosis. For physicians, an in-office WBCT is also more convenient, enabling quicker treatment plan formulation, helping to avoid overbooking, while allowing for more rapid surgery scheduling.
Dr. Cuttica reviewed three office workflow options for in-office WBCT imaging:
Option A – Scan and have patient follow up to go over scans at a later date (not the most efficient)
Option B – Get insurance authorization and perform the scan at the next visit before the patient is seen
Option C – Get insurance authorization, perform the scan, and go over scans at initial appointment (most efficient and most convenient for patients)
Further, WBCT images can be conveniently emailed or uploaded to another doctor or radiologist.
Dr. Cuttica said the most common and beneficial WBCT foot and ankle applications include:
Hallux valgus
Pes planovalgus
Midfoot/Lis Franc injury
Ankle fracture/syndesmosis
Deformity/Charcot
OCD
Bone healing
In Hallux Valgus, WBCT Scans Accentuate Deformities & Guide Treatment
(17:03) In hallux valgus—a triplane deformity—it’s necessary to understand all the components of the malformation. Dr. Cuttica pointed out that WBCT allows for better understanding of coronal plane rotation. As you can see in the image below (17:40), the WBCT imaging clearly shows the first metatarsal joint architecture, the sesamoid position, if there is any flattening/erosion of the crista, as well as a first metatarsal rotation, all of which need to be taken into account when treating bunion deformity.
This screen capture from Dr. Cuttica’s FOOTInnovate webinar displays rotation of the first metatarsal.
(18:16) Dr. Cuttica displayed a typical case of a 47-year-old female with bunion pain who, upon both exam and radiographically, had a hypermobile first ray with some inter-gapping at her first tarsal-metatarsal joint, as well as a moderately sized bunion. (19:43) When Dr. Cuttica performed a WBCT, the rotation of her first metatarsal was visible. Due to the patient’s instability and hypermobility at the joint, Cuttica’s team treated her with the Lapidus procedure—correcting her IM angle and coronal frontal plane rotation—as well as an Akin osteotomy.
(19:55) At the 6-week post-op exam, the patient’s foot looked fairly healed, and allowed the patient to progress with some activity. (20:19) At the 12-week exam, however, an additional WBCT allowed Dr. Cuttica to better assess the sesamoid position and evaluate the fusion. The sesamoids looked reduced, but it was also revealed that the patient was not fully fused.
This screen capture from Dr. Cuttica’s FOOTInnovate webinar shows the sesamoid position has improved post-operatively.
However, this screen capture from Dr. Cuttica’s webinar revealed the patient’s bones had not fully fused after undergoing a lapidus procedure.
These comprehensive views enabled Dr. Cuttica to better progress with the patient’s treatment—in this case, limiting the patient’s activities as she had a bit more healing to go.
Many have long thought that the means of assessing osteoarthritis in the knee are less than ideal.
Although conventional X-ray radiographs are widely considered as gold standard for the assesssment of knee OA, in clinical and scientific settings they increasingly bare significant limitations in situations where high resolution and detailed assessment of cartilage is demanded. – Wick et al, Gereontology. 2014; 60(5).
Current standard of care consists of a series of X-rays on a routine interval basis to assess whether disease is progressing further and corresponding with the patient’s symptoms. There is questionable reliability of joint space width (JSW) measurements from X-ray, and it is difficult to decipher whether there has been a significant change in anatomy to explain the patient’s worsening symptoms.
Watch the video to see a bilateral weight bearing CT dataset of a patient with osteoarthritis in his knees.
CurveBeam’s cone beam CT technology offers high resolution, axial, coronal, and sagittal views in 0.3mm slices generated from a 30 second scan. This provides 3-dimensional, weight bearing information with radiation exposure levels almost equivalent to the standard series of knee X-rays. The 30 second scan is much faster for the technician to acquire compared to the back and forth for multiple views in an X-ray series.
Incorporating weight bearing CT technology into daily practice could facilitate complete visualization of the joint surface in axial slices and take into consideration the effects of weight bearing at the joint line. In time, clinicians should be able to provide more detailed information on location and progression of disease for their patients, and therefore, determine the best course of care moving forward.
In this episode of the CurveBeam podcast, host Vinti Singh sat down with Dr. Martinus Richter, MD, Ph.D.to discuss the results of his latest published study: “Results of more than 11,000 scans with weight-bearing CT – Impact on costs, radiation exposure and procedure time.” This first-of-its-kind study examined the economic implications of CT scans versus radiographs for patients.
Click here to download the execuctive summary for this episode of CurveBeam Connect, featuring Dr. Martinus Richter, MD, PhD.
Dr. Richter is department head of the foot and ankle orthopedic surgery section at Hospital Rummelsberg in Rummelsberg, Germany and has published numerous studies in orthopedic journals.
Dr. Richter oversaw a study, which was conducted over more than five years. to assess the benefits of using weight bearing CT (WBCT) instead of a combination of weight bearing radiographs (R) and conventional CT (CT). The study looked at the modalities’ impacts on costs, radiation exposure and procedure time.
In the study, 11,009 scans, taken from July 2013 through March of 2019, were obtained from 4987 patients—45% (4,897) before treatment; 55% (6,022) at follow-up—with a yearly average of 1,957 WBCTs (bilateral scans). These were compared to 1,850 Rs (bilateral feet, dorsoplantar and lateral, metatarsal head skyline view) and 254 CTs obtained from 885 patients (RCT group) in 2012.
The conclusions help to solidify that not only can WBCT more precisely measure bone position than conventional R and CT scans, but also decreases the time needed for image acquisition by 77% and radiation dosage by 10%, while increasing institution financial profitability by $57.19 (51€) per patient.
CT assessment of patients casted for a non-displaced scaphoid fracture shows union occurring at approximately 7.5 weeks, with a majority of fractures healing in less than 6 weeks, according to a 2016 study by Ruby Grewal et al. Similar studies using plain X-Ray demonstrated union time to be anywhere between 10 – 24 weeks. The authors noted the union time on CT may even be overestimated because the majority of patients’ first CT scan after casting was not until 6 weeks.
The CurveBeam InReach provides 0.2mm high resolution slices of the distal limbs.
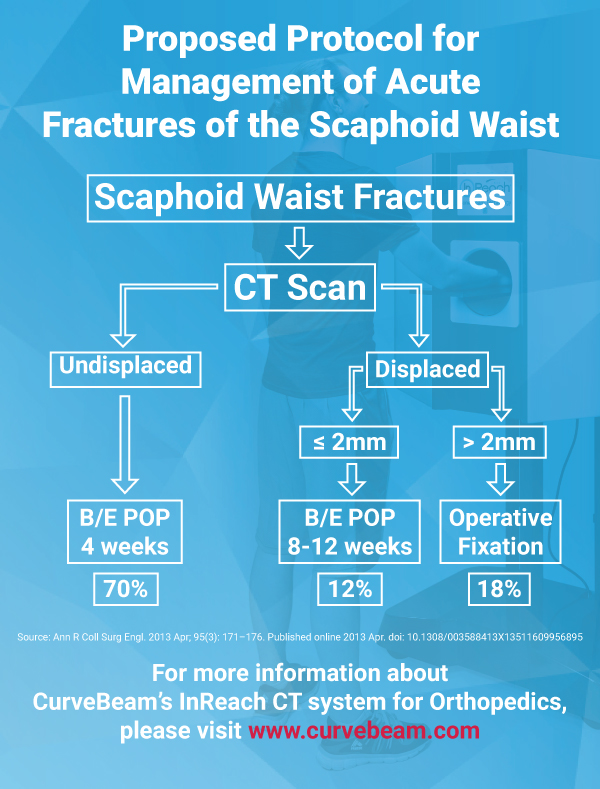
In a previous study, Professor Timothy Davis wrote CT studies demonstrate healing of a non-displaced fracture treated with a plaster cast can occur in as little as 4 weeks. If a fracture is displaced less than 2 mm, Davis said those CT studies suggest a plaster cast for 8 – 12 weeks.
CT is ideally performed for all scaphoid waist fractures in the first week after injury to classify whether they are displaced or non-displaced, said Professor Davis, an orthopedic surgeon at Woodthorpe Hospital in Nottingham, UK said in his research paper.
Professor Timothy Davis proposes the above workflow , which calls for a CT scan for every suspected scaphoid waist fracture.
By using CT as a baseline, researchers at the Roth/McFarlane Hand and Upper Limb Center in London said they were able to identify fractures which may have appeared non-displaced on X-Ray, but were actually minimally displaced.
“We feel that the added visualization of CT over plain radiography enables the surgeon to properly select which fractures are appropriate for non-operative cast treatment with an expected high degree of union,” the researchers said in a study published in The Open Orthopaedics Journal.
Out of the research setting, routine CT scans of scaphoid fractures may not be practically feasible, Professor Davis wrote.
“I appreciate that [routine CT assessment of scaphoid fractures] is impossible in many centers at the present time but it should become increasingly possible in the future,” Professor Davis wrote in the medical journal “Annals of the Royal College of Surgeons of England” in 2013.
The CurveBeam InReach plugs into a standard wall outlet and is self-shielded.
The InReach is a compact CT imaging system dedicated to the hand, wrist and elbow. The system received FDA and CE approval in 2017. Since then, it has been installed in leading orthopedic centers and hospitals in the United States. The InReach allows orthopedic practices to offer CT imaging at the point-of-care.
“InReach has been an excellent asset allowing in-office imaging and rapid CT evaluation of the hands with complex diagnostic dilemmas,” said Dr. Lloyd Champagne, an orthopedic surgeon at the Arizona Center for Hand to Shoulder Surgery in Phoenix.
Fifteen percent of acute fractures of the scaphoid waist fail to unite if treated non-operatively in plaster, resulting in a persistent loss of function, according to the 2013 article. Plain X-Rays do not clearly show fracture features such as displacement and communition. Previous inter-observer studies have shown radiographs of scaphoid fractures are neither sensitive nor specific.
For professional athletes, injuries mean reduced playing time, impacted performance, and, in rare cases, an end to their careers. These injuries often affect the lower extremities, primarily because their sports require high-risk activities like jumping, cutting movements, and collision with other players. While traditional scanning techniques have mainly been used to identify injuries, a recent study found that weight-bearing cone beam computed tomography (CBCT) may be crucial to not only identify anatomic risks but also to help develop treatments explicitly tailored to the needs of professional athletes.
Incorporating new tech
In The Orthopaedic Journal of Sports Medicine, Dr. Cesar de Cesar Netto, et al. examined the morphology of foot injuries in 45 active NBA players. The doctors used weight-bearing CBCT scans to obtain 3D imaging of each foot. These scans provide more accurate alignment measurements than traditional scans and offer views of the foot while the player’s natural weight is being placed on it.
The study sought to discern whether the morphology of NBA players differed from that of the population at large, and whether the morphology changed based on position played. Foot and ankle injuries account for 27 percent of professional sports injuries, and 85 percent of basketball players experience at least one ankle sprain in their career.
Getting a better look
The players who participated in the study ranged from 20 to 31 years of age, and in total 29 right feet and 25 left feet were studied. All images were taken using a state-of-the-art pedCAT CurveBeam pedCAT system to obtain reliable and accurate images of each subject, and measurements were taken both manually and using the automatic TALAS measurement tool included with CurveBeam’s CubeVue software. TALAS is a research tool and is not available for clinical use. This is significant as it is the first time that a study of the foot morphotypes of NBA players has been conducted.
The study found that, for the most part, NBA players have standard alignment in their lower extremities, although they do tend to have high arches and varus hindfoot alignment. These trends were slight, but they are related to foot injuries and should still be noted. Building up a database of weight-bearing CBCT scans of professional athletes could also allow specialists to have a new control group to compare scans to, which would be enormously beneficial., the study authors said.
Better analysis means better results
Incorporating weight-bearing CBCT scans like those of CurveBeam’s pedCAT can save players, and the league as a whole, both time and money in the long term. Not only will they be able to watch for warning signs, but they will have a complete view of available injuries and will could develop more specific training regimens geared towards returning athletes to the court as quickly as possible.
You can read the full study by Dr. de Cesar Netto, et al. here.

















{kind=link}